

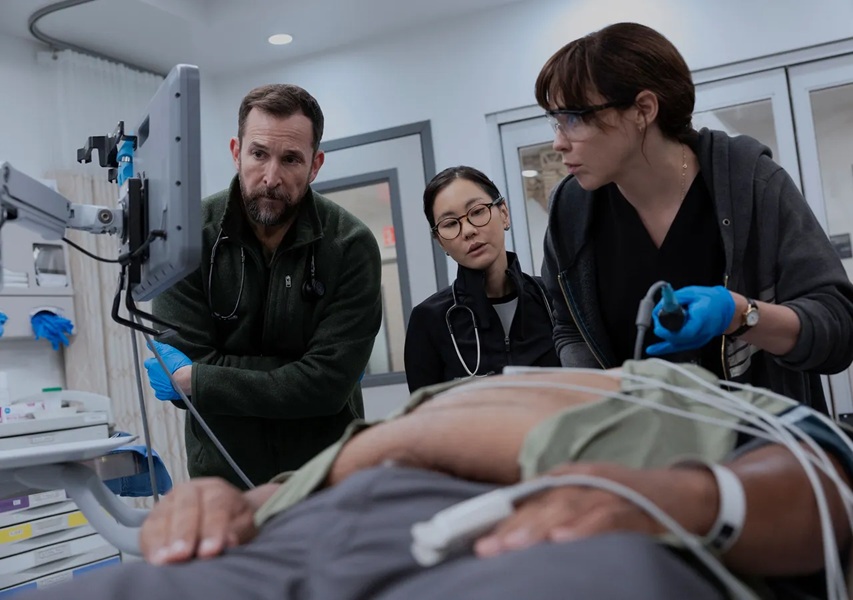
It is early in the morning at what appears, from a distance, to be a functioning hospital in Pittsburgh, Pennsylvania. A teenager has just been brought in by ambulance, unresponsive, fentanyl on board. In the waiting room, which has been full since before the first patient of the day arrived, a woman is pretending to be more sick than she is, for reasons that will not become clear for another two hours. A charge nurse named Dana Evans is doing four things at once with the practiced efficiency of someone who has been doing four things at once for most of her professional life. And Dr. Michael “Robby” Robinavitch, the department’s senior attending physician, is standing at the center of all of it — calm, watchful, conducting the chaos of his emergency room the way a musician holds a difficult piece of music in their head all at once, hearing every instrument even when they’re not playing.
This is the opening hour of The Pitt, HBO Max’s defining medical drama, and if you have watched it, you probably remember exactly where you were when you realized you were not going to stop.
The show premiered on January 9, 2025, to reviews that ran out of adjectives inside the first week. It has since won five Emmy Awards, including Outstanding Drama Series. It took the Golden Globe for Best Drama. Its second season, which began airing in January 2026, is running a 99% approval rating on Rotten Tomatoes — a number that inspires the same mild suspicion as a unanimous vote, until you watch it and find yourself thinking, yes, all right, I understand. By any measure that the television industry uses to track such things, The Pitt is a phenomenon. What is harder to articulate — what critics have reached for in various directions without quite landing — is the precise mechanism of its hold on the people who watch it. Viewers and critics alike are constantly asking why The Pitt is so engaging, and the answer lies in its unique immersive quality.
Some shows you admire. Some you enjoy. Some you watch because everyone is watching them and you do not want to be left out of the conversation. The Pitt does something rarer, and more specific. It makes you feel like you are somewhere else.
Not transported in the escapist sense — not deposited into a fantasy or a thriller or anywhere you would particularly choose to be. Transported in the way that the best journalism sometimes works, or the best documentary: you find yourself somewhere you did not expect, among people whose lives you had not previously imagined in detail, and the experience changes the texture of the hours afterward, the way any genuine encounter does.
Noah Wyle was not planning to do this again. After eleven seasons as Dr. John Carter on ER — which, at its peak in the mid-nineties, was drawing nearly forty million viewers an episode and had made Wyle, along with his castmates, into a species of celebrity that the streaming era has largely rendered extinct — he had made a decision. No more doctors. “I spent fifteen years actively avoiding walking down what I thought was either hallowed ground or traveled road,” he said, in an interview with NPR earlier this year. The stethoscope stayed in the drawer. He did genre television, science fiction, an adventure series. He did not play anyone in scrubs.
Then the COVID-19 pandemic happened, and his inbox started filling up.
The messages came from nurses and paramedics and emergency room physicians, and they came in a volume that Wyle had not anticipated. They were not, primarily, fan mail — or not only that. They were dispatches from a world under extreme pressure, written by people who needed somewhere to put what was happening to them and had, for reasons that Wyle found both touching and unsettling, chosen to put it there. Many of them told him that ER had inspired them to enter medicine. Now they were working through something that medicine had not prepared them for, and they were exhausted, and they were frightened, and they wanted him to know.
He shared the messages with R. Scott Gemmill and John Wells, his former collaborators, the people he had spent a decade and a half making television with. The three of them had stayed in touch in the years since ER ended; they ran into each other at parties, kept up the mild, affectionate contact of people who have made something good together and not quite forgotten it. What Wyle showed them changed the tenor of those conversations.
“We realized that there was a reason to do it again,” Gemmill told Variety, “as long as we could find a way to do it that was fresh for both us and the audience so that we weren’t just retreading what we’d done in the past.” Wells was more direct about what had shifted. “There’s some significant problems,” he said. “It seemed like within the context of trying to follow someone through an entire day, you could actually touch on just how difficult being in these urban medical settings are now.”
This is how The Pitt began: not with a network pitch or a streaming deal, but with a stack of messages from overwhelmed healthcare workers and three people who had made a great medical drama once and thought they might know how to make a different kind of one.
The format they settled on is so elegantly simple that it is worth pausing on before going further, because it is the hinge on which everything else turns and a key reason why The Pitt is so engaging.


Each of the season’s fifteen episodes covers one hour of a single shift. The episodes are titled with the time: “7:00 AM,” “8:00 AM,” and so on, through “9:00 PM.” What this means, in practice, is that the viewer spends fifteen weeks — one episode per week, released Thursday evenings on HBO Max — watching one day in one emergency room in Pittsburgh, Pennsylvania. No time-jumps. No “two months later.” No clean slates. When a patient arrives in hour two, they may still be in the building in hour eleven, changed or unchanged, improving or not, their family wearing the specific exhaustion of people who have been waiting in a hospital for nine hours. Whatever is unresolved at the end of one episode is unresolved at the start of the next, because there has been no gap for resolution to happen in.
It sounds like a constraint. It is, in fact, a liberation — or at least, it liberates the show from the specific gravity that has always made the medical drama a slightly falsifying genre. The standard model of the hospital show is built around compression. Time skips. Problems that were impossible on Tuesday are, by Thursday, soluble or at least evolved. Characters can have breakdowns, recoveries, affairs, and reconciliations in the ellipsis between episodes, arriving each week refreshed and newly complicated. The machinery of drama is serviced, oiled, reset.
The Pitt refuses to reset. The machinery runs hot the whole time, and what breaks starts to show.
Wyle compared the experience, in an interview, to being embedded with a military unit. “It’s somewhat analogous to being like a combat correspondent, embedding yourself within a unit for a period of time,” he said. “That fully realized experience is only going to be had that way.” The analogy is apt, and not only for the obvious reasons. Embedded journalism works not because the reporter is objective — they are not, they cannot be — but because duration produces a kind of understanding that brief access never achieves. You learn, over time, the texture of a place. The habits, the frictions, the private language that develops among people who spend their days inside the same pressurized environment. The Pitt uses its fifteen-hour structure to earn exactly that kind of understanding. By hour seven, the viewer knows the ER the way a new hire knows it after a month: the rhythms, the shortcuts, the specific weight of Dana Evans’s silences.
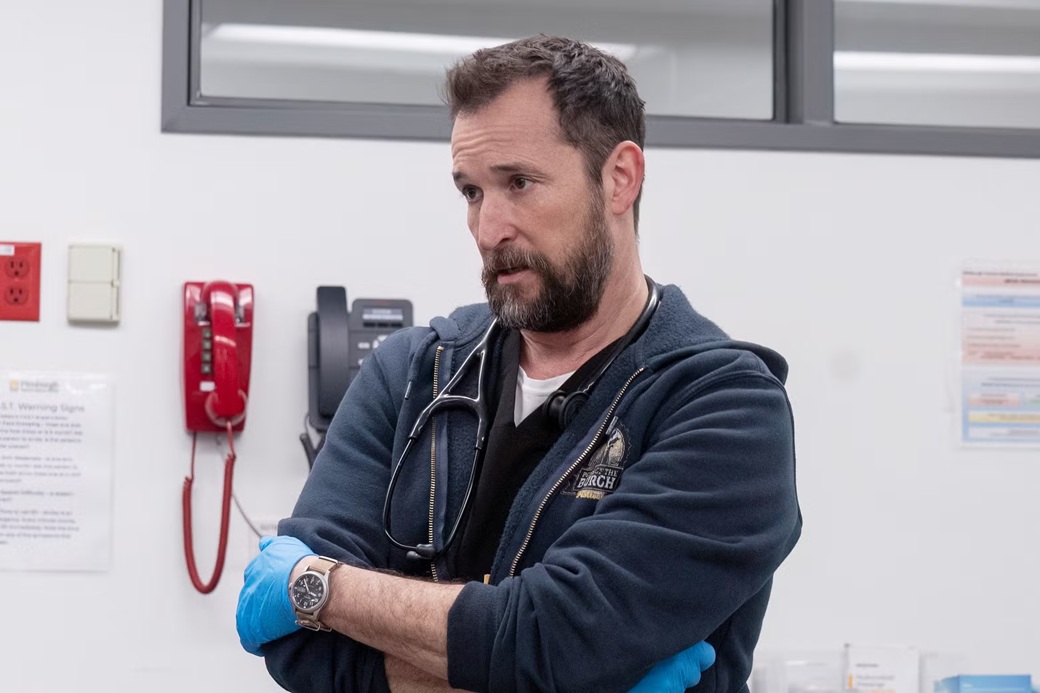
Wyle plays Robby as a man carrying more than one shift’s worth of weight. The first season is set on a specific day — the fourth anniversary of the death of Robby’s mentor, Dr. Adamson, whom he lost in the early weeks of the COVID pandemic under circumstances that the show withholds, then parcels out in fragments across several episodes. It is, for Robby, the worst possible day to go to work. It is also the day he chooses, out of some combination of duty and the particular stubbornness of people who have survived things by refusing to stop functioning. The PTSD he is managing — and “managing” is the right word, with all its connotations of ongoing effort and partial success — surfaces not in dramatic confession but in the body, in small involuntary responses that the camera catches and does not comment on.
Before they began filming, the production team made a decision about how to introduce Robby. There would be no establishing shot of his apartment, no morning routine, no personal context offered before the shift begins. The show meets him on the street, walking to work. That’s all.
“Every choice you make from the second you establish him is going to define him in a way that will either relate him or not relate him to an audience member,” Wyle explained. “You don’t over-define him in a way, and you don’t under-define him. You just have to present them and let the circumstances play themselves out.”
What this produces, over fifteen episodes, is a portrait assembled from professional behavior. Because we have no access to Robby’s life outside the building, every glimpse of his interior — a flinch, a pause held slightly too long, the way he says a patient’s name — carries a weight that backstory would dilute. We are always in the process of learning him. The sense of incompleteness is not a failure of characterization; it is the characterization. People are not fully legible. In the context of an emergency room, where everyone is running on reduced resources and professional composure is the social contract, they are even less so.

The Emmy that Wyle received — Outstanding Lead Actor in a Drama Series — was not the kind that rewards the memory of a career. It was earned, specifically, in a sequence toward the end of the season in which Robby’s accumulated exhaustion and grief finally exceeds his capacity to contain it. The scene takes no shortcuts. It arrives as the natural consequence of everything that has been building across thirteen hours of television, and Wyle meets it with a physical honesty that doesn’t announce itself as method acting. It simply happens, and you find yourself in the strange position of feeling that you have watched someone break down rather than a performer simulate one.
Katherine LaNasa, who plays the charge nurse Dana Evans, won an Emmy too. This is worth dwelling on, because the show’s relationship to the nursing staff is one of its most unusual qualities.
Medical dramas have traditionally organized themselves around physicians. Nurses appear, dispense medications, relay information, occasionally have a subplot of their own. They are the supporting structure, treated as such. In The Pitt, the first thing Robby does when introducing the new interns to the department is point to Dana. “This is the most important person you are going to meet at this hospital,” he tells them. He is not being gallant. He means it functionally, operationally, and the show proceeds to demonstrate why. Dana knows where every supply is, which patients are flagging before the monitors catch it, which physicians have which tendencies under pressure. She is the department’s institutional memory, its connective tissue.
LaNasa plays her without softening the edges. Dana is exacting, occasionally alarming, always right. She is also, beneath the professional armor, carrying her own version of the weight that everyone in the building carries — the specific exhaustion of someone who has been required to give more than is reasonable for longer than is sustainable. The Emmy was, in a sense, a recognition of something the show had done deliberately: make visible the labor that is usually rendered invisible.
Wyle has described The Pitt as fundamentally “provider-centric,” in contrast to ER, which he sees as having leaned more toward the patient’s perspective. It is a fine distinction, but a meaningful one. A provider-centric show is not necessarily a show that flatters its providers; it is a show interested in what the job actually does to the people who do it. What it costs, what it gives back, what it requires you to suppress and what it makes possible.
Khullar, who has spent his career thinking about both sides of that transaction, finds this orientation one of the show’s defining qualities. Good care, he is quick to point out, “almost always requires the hard, often unglamorous work of many people over many days.”
His complaint about most medical dramas is what he calls the Great Man theory of medicine — the cowboy surgeon, the diagnostic genius, the lone brilliant physician cracking an impossible case and saving the day. The Pitt has a touch of that, he acknowledges. But more often, it tells a truer story. Medicine is a team sport, and the team is the point. This focus on team dynamics over individual heroics is part of why The Pitt is so engaging to those in the field.
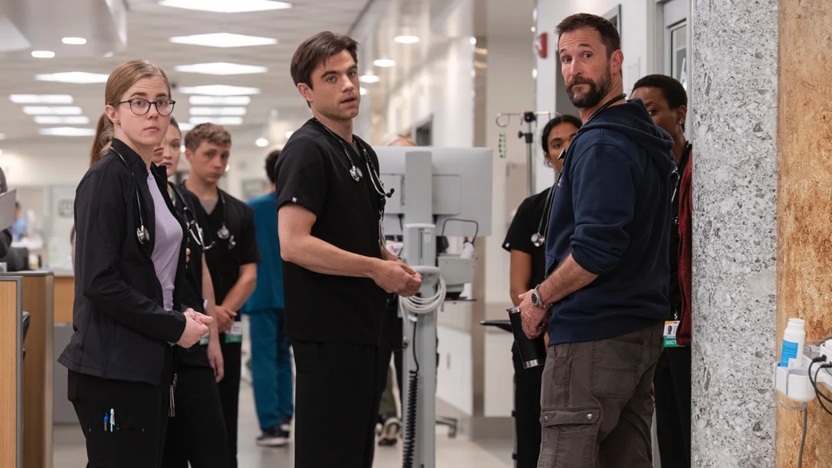
The rest of the ensemble is built with similar attention. The residents and interns — each at a different stage of initiation, each with a different relationship to the gap between what medicine asks and what they have to give — create a kind of gradient across which the audience can watch competence and self-knowledge develop in real time. Dr. Cassie McKay, played by Fiona Dourif, is managing something in her past that the show reveals slowly and without fanfare. Dr. Heather Collins, played by Tracy Ifeachor, is a senior resident whose undisclosed pregnancy creates an undertow beneath her professional confidence. Dennis Whitaker, a medical student played by Gerran Howell, is consistently, endearingly overwhelmed — the character who most clearly mirrors the audience’s own position, always one step behind the pace of the building he’s learning to inhabit.
Before filming began, the cast spent two weeks in what Wyle described as a medical boot camp. They worked with emergency room physicians — learning suturing, intubation, CPR, the physical choreography of a trauma bay. The extras received training, too. John Wells, who directed the pilot and executive produced the series, told Wyle early in the process: “Don’t be too nice to them.” He then separated the actors by rank, so that the isolation of the medical hierarchy was felt before the cameras rolled. Wyle ate alone. The residents sat together. The students clustered. By the time they entered the set, they already knew, in their bodies, what it felt like to be in the room.
The hospital itself deserves consideration.
It is, technically, a soundstage in Burbank, California — eighteen thousand square feet at Warner Bros. Studios. But the production designer built it without the usual accommodations for filmmaking: no removable walls, no dedicated camera positions, no places for crew to stand and observe while an actor hits a mark. The crew navigated the space as though it were real, ducking into unused exam rooms, finding angles in corridors, occasionally being caught in a reflection through an interior window. The medical equipment came from manufacturers who supply actual hospitals. The nurses’ station was designed and built from scratch to exact specifications.
Zoë Ruscio, the production designer, used marble columns at the ER entrance as a deliberate metaphor: the emergency room as the basement that holds up everything above it while bearing the full weight of the structure. It is the kind of architectural thinking that most television design ignores entirely, because most television design is not trying to make you feel something before anything has happened. Here, before a single patient arrives, the space is already telling you something about what the work is like.


The show uses almost exclusively practical effects — prosthetics, makeup, physical simulation — with minimal post-production adjustment. The company Autonomous FX built the prosthetics. The sound design is calibrated to produce a specific quality of overwhelm: multiple simultaneous conversations held at the precise threshold of comprehensibility, machines providing an insistent electronic underscore, the acoustic signature of a place where everything is urgent and nothing is quiet. Some critics compared the sensory texture to the Safdie Brothers’ films — the kinetic, close-quarters intensity of Uncut Gems, the sense of a camera that is always too close to something uncomfortable. The comparison is not wrong. Both share a commitment to using the physical environment to produce a psychological state in the viewer, not merely to illustrate one. This sensory overload is a critical component of why The Pitt is so engaging.
What the show is actually about — beneath the format, beneath the excellent acting, beneath the production design that keeps tricking your nervous system into thinking you’re actually in an emergency room — is something that is easier to feel than to name.
It is about what the pandemic did to American healthcare workers and what American healthcare did to them before that. It is about the specific demoralization of a profession that was asked, for years, to absorb the consequences of systemic failure and simply continue showing up. Wyle has said, in various interviews, that none of this would exist without COVID — not the show, not his willingness to return to medical drama, not the particular quality of urgency that runs through every episode. “That was the catalyst for all of this,” he told one interviewer. “That post-COVID, there might be another story to tell about American healthcare that shined a light on the two different healthcare systems that exist in this country, the disparity between the two, and the toll that it was taking psychologically, emotionally and financially on the frontline workers. Without COVID, there would’ve been no need for me to put a stethoscope on my neck ever again.”
The resulting show is, perhaps surprisingly, not polemic. It does not deliver speeches about healthcare policy. It does not have a villain who represents the insurance industry or a hero who defeats the system through ingenuity. What it does, instead, is show the conditions. The waiting room that has been full since before the shift started and will be full long after it ends. The psychiatric consult that Robby cannot get, not because anyone is cruel but because the resource doesn’t exist in the quantity the building needs it. The nursing shortage that means Dana is managing a department with fewer people than it requires, which is not a problem that arrived this week or will be solved by next. The opioid crisis that sends patients in one after another, not as individual tragedies but as the visible face of something that runs through the city like a current.
Board-certified emergency physicians have written at length, in various public forums, about the accuracy of the show’s rendering of these conditions. One, who described having spent years avoiding medical television because of its distortions, said that The Pitt was the first show she had encountered that captured “the reality of ER medicine as well as hospital politics.” Another, still practicing, said it helped him remember why he had entered the field — that it reminded him of the part of medicine that gets lost when everything else is demanding your attention.
Dhruv Khullar, a physician and contributing writer at New Yorker, has been thinking about why the show resonates differently from its predecessors. He is not, he is quick to say, especially interested in whether the medicine is technically accurate. “I’m less concerned with whether a show is technically accurate than whether it captures the human aspects of medicine,” he told me recently. What The Pitt captures, in his view, is something harder to fake: the texture of what it actually feels like to work inside a broken system while still finding, within it, the reasons you chose it. “There’s this ever-present awareness that the system is broken and the work is endless,” he said, “and yet there are moments of deep humanity to be found. Those moments are why many of us went into medicine.”
The distinction he draws is quietly important. Technical accuracy is a craft problem — hire good consultants, rehearse the procedures, get the jargon right. What The Pitt achieves is something different. You cannot watch a full season of it, Khullar observed, without arriving at a more honest understanding of what patients actually endure — the waiting, the fear, the insurance paperwork, the feeling of navigating a system that was not, in any meaningful sense, designed with you in mind — and what the people on the other side of the curtain endure in kind.
The show, to its considerable credit, does not ask you to simply admire these people. It asks you to understand them, which is different — harder, and more durable. Admiration is a posture. Understanding is something you carry.

There is a scene in the third episode of the first season in which a Black woman with sickle cell disease arrives in the emergency room in acute pain and is, by a senior physician who is not Robby, initially treated as drug-seeking. The scene does not editorialize. No one delivers a monologue about implicit bias in medicine. The physician who makes the initial call is not a villain; he is a human being in a busy emergency room, operating on reflexes that the environment has shaped. The show holds this with a steadiness that is harder to achieve than it looks, presenting the interaction as what it is — routine, structural, the kind of thing that happens in emergency rooms every day — without asking the audience to locate it anywhere other than the room in which it occurs.
This is The Pitt‘s method throughout. Its social commentary, and there is social commentary, is delivered not through character but through condition. You understand what the opioid crisis looks like in an emergency room not because someone tells you, but because you watch the third patient in two hours arrive via ambulance, and you have been in this building long enough to understand what the department’s resources look like after two hours, and you do the arithmetic yourself.
“We wanted to talk about what heroes they are again,” Wyle said, of the healthcare workers the show depicts. “Not just in a ‘Let’s clap for them as they finish their shift and save our lives’ way. But in a real, empathetic way and show the world what it’s like to walk in their shoes.” The distinction between those two kinds of attention — the appreciative gesture and the sustained act of understanding — is what separates The Pitt from the genre it nominally inhabits.
At the mid-century, the television network understood something that streaming has spent a decade arguing itself out of: the audience wants to gather.
There is a specific pleasure in watching something at the same time as everyone else — in knowing that the cliffhanger you encountered on Thursday night is the cliffhanger that six other people you know also encountered Thursday night, and that you have a week to think about it together before the next installment arrives. Streaming, with its full-season drops and its algorithms calibrated for the binge-watching, evacuated this pleasure in the name of abundance. You could watch whenever you liked, as much as you liked, at whatever pace suited you. The result, perhaps predictably, was that fewer shows became cultural events. A program could be watched by millions and still feel, in some diffuse way, private — an experience consumed rather than shared.
Casey Bloys, the head of HBO Max, had been thinking about this problem when he greenlit The Pitt. He wanted, he later explained, a show that would keep an audience engaged over a longer period — one that would recreate the conversational culture that appointment television had once generated. The show would run fifteen episodes, released weekly, on Thursday evenings at nine. No full-season drop. No overnight availability. Come back next week.
The decision looked counterintuitive. In practice, it turned out to be the show’s second structural masterstroke. The real-time format creates one kind of collective experience — you live through the shift alongside the characters — and the weekly release creates another. Between episodes, the audience carries the unresolved situations with them. What is going to happen to the patient who arrived in hour twelve? What will Robby do with the piece of information he received at the end of hour eight? The show gives you a week to think about it, which is also a week to talk about it, argue about it, recommend it to someone who has not yet seen it.
The budget, too, shaped the form. Each episode cost between four and six million dollars — modest by prestige television standards, which made it possible to order fifteen of them. The economics and the aesthetics are, in this case, genuinely inseparable. The Pitt is the show it is partly because it could not be made for the prices that demand a shorter, more expensive, more conventionally prestige season. The constraint made the format. The format made the show.
At some point in the middle of the season — hour seven or eight, perhaps, somewhere in the long afternoon of the shift — something changes in how you are watching, and you begin to understand why The Pitt is so engaging.
It is not that the show gets better, though it does deepen. It is that the accumulation of hours has produced something that television usually cannot produce: the sense of having actually been somewhere. You know the layout of the department. You know which bay tends to get the traumas, where the supply closet is, the sight lines from the nurses’ station. You know that when Robby goes to the roof, it means something specific. You know Dana’s tells. You know, watching the clock in the corner of the screen tick toward the late afternoon, that the shift is getting harder to sustain — that the people who were tired in hour four are now something past tired, operating in that diminished state that the body enters when it has exceeded its reasonable limits and is running on obligation alone.


The exhaustion is, in the truest sense, shared. Viewers have described the experience in terms you rarely hear applied to prestige television — depletion, the feeling of needing to sit quietly for a moment after an episode, the odd solidarity of having lived through something alongside characters you have come to know.
It is not comfortable viewing. It is not supposed to be. The shift is meant to be worked, and by the time the final episode ends, you have, in some experiential sense, worked it.
Wyle, who has given, by his own estimate, over a hundred interviews since the show premiered and does not enjoy the process, talks about the letters he receives from viewers with a different quality of attention. “People don’t just want to tell me that they enjoy it,” he said in an interview with The Wrap. “They want to tell me that it affected them and resonated with them in a way that was very personal. Maybe it was a storyline involving losing a loved one or a parent, or maybe they knew somebody who had experienced the tragedy of a fentanyl overdose.”
This is the transaction the show is actually conducting, beneath the procedural machinery and the technical accuracy and the structural ingenuity. It is offering to take the viewer somewhere real — not a fantasy of what emergency medicine could be, not a morality play dressed in scrubs, but a genuine rendering of a world that most viewers have encountered only as patients, and only in the fragmented, anxious state in which patients encounter it. The Pitt gives you the view from the other side of the curtain, held for long enough that you can understand what it costs.
It would be possible to discuss The Pitt without discussing ER for approximately four paragraphs before the evasion became too obvious to sustain. Wyle was Dr. John Carter for eleven seasons and two hundred and fifty-four episodes. Gemmill was an executive producer on ER‘s later seasons. Wells ran the show at its peak, in the nineties, when it was one of the most watched programs in American television history. The lineage is not merely acknowledged; it is the origin story.
But the two shows are, in the ways that matter, quite different, and the differences are instructive.
ER was organized, as most network medical dramas were and are, around the personal lives of its physicians. Romance, rivalry, breakdown, recovery — the medical cases provided the context in which these human dramas played out. The hospital was a container for personal drama. The heroism was of the individual variety, brilliant doctors making brilliant calls, occasionally at cost to themselves. The systemic was always present in ER, but it was always background; the foreground was people.
The Pitt inverts the hierarchy. The systemic is structural. Everything that happens in the ER happens within and because of conditions that no individual can alter, however competent or dedicated. Robby cannot diagnose his way out of an underfunded department. Dana cannot will adequate nursing staff into existence. The opioid epidemic is not a backdrop for a meaningful patient story; it is a feature of the environment that determines how the day unfolds. The personal — Robby’s grief, Collins’s pregnancy, McKay’s history — surfaces within these conditions and is shaped by them. People matter enormously, but they matter as people, not as exceptions to the systems that contain them.
This is, arguably, a more mature relationship with the genre than ER achieved, and Wyle is frank about the difference. “We pivoted as far in the opposite direction as we could in order to tell the story we wanted to tell,” he said, of the deliberate choice not to simply recreate what they had made before. The point was not nostalgia. The point was that the story had changed, because the world the story was about had changed, and making the same television in response would have been a failure of attention.
The last time Wyle was at the center of something like this — a cultural phenomenon, the specific gravity of a show that everyone is watching — was the mid-nineties, and he was twenty-three years old. He had driven through the same gate at Warner Bros. studios that he drives through now, and entered a version of the same world, and emerged on the other side famous in a way that took years to metabolize.
This time, he said, is different in character if not entirely in scale. “I had gotten my anonymity back and was comfortable with it,” he told The Wrap. “And now it just feels lovely to have people shout out, ‘Hey Robby, love the show!’ It’s maybe less in volume and a bit more in earnest, if that makes sense.”
He is fifty-three now, an executive producer and writer on the show as well as its star. He has described the experience of returning to this world — the gate, the studio, the scrubs, the stethoscope — as “extremely synchronistic,” a word that suggests something more than coincidence without claiming to understand it. What he seems to mean is that the pieces arrived in an order that made sense only in retrospect: the pandemic, the messages, the reunion with Gemmill and Wells, the format that emerged from their conversations, the show that no one, including the people making it, expected to land with this much force.
The second season is running now, its shift set on the Fourth of July, a year into Robby’s story. A new medical student joins the department. Two colleagues return from time away. The clock starts again at 7:00 AM, and the waiting room fills, and Dana takes her position at the nurses’ station, and whatever the day will bring begins its approach.
It is a Thursday evening on HBO Max. People are gathering, reminding us once again why The Pitt is so engaging.